This Non-Drug Therapy Could Replace Opioids for Pain Management
MossRehab is the first in the region to use the SPRINT endura Peripheral Nerve Stimulation (PNS) System, a promising new therapy for acute and chronic pain.

The SPRINT endura Peripheral Nerve Stimulation (PNS) System is a recently FDA-approved treatment for acute and chronic pain. / Courtesy
As the clinical director of neuromodulation services at MossRehab, Michael Saulino is always looking for new ways to treat nerve pain in patients that don’t involve addictive opioids.
“When it comes to neuropathic pain, opioids are not very effective at all,” Saulino said. “Patients often wind up being dependent on it, not because of their pain relief qualities, but just because of the addictive nature of the medication.”
When Saulino learned about a new, minimally invasive nerve stimulation therapy last year, he jumped at the opportunity to offer the treatment to Moss patients.
Saulino is the first physician in Philadelphia to use the SPRINT endura Peripheral Nerve Stimulation (PNS) System, a recently FDA-approved treatment for acute and chronic pain. MossRehab is the only facility in the region that currently offers the 60-Day implant treatment that does not require surgery, incisions or anesthesia. Studies show that pain relief is sustained after the implant is removed. Saulino says it’s a welcome option for stroke patients who typically have to choose between less effective treatment options like antidepressants, anticonvulsants, and injection therapies that come with a host of side effects.
Saulino has used the SPRINT system to treat several post-stroke shoulder pain patients. So far, half of the patients Saulino treated have eliminated their pain medications completely and the other half of patients have reduced their medication. All of Saulino’s patients reported greater than 50 percent relief, including Peterson Saintvil.

Peterson Saintvil, 30, was one of the first patients to receive the SPRINT system therapy at Moss.
Ten years ago, Saintvil experienced a slip-and-fall accident that caused him to have a stroke and required that he undergo spine surgery at the young age of 20. Despite having an intrathecal pump — a device that delivers pain medication such as morphine via spinal fluid — Saintvil continued to struggle with post-stroke shoulder pain. An orthopedic doctor told him surgery was his only hope for pain relief. Another doctor Saintvil visited for a second opinion sent him home with a prescription for Oxycontin, the highly addictive pain medication with side effects like respiratory failure and death.
Saintvil didn’t like any of the treatment options he’d been offered.
“I didn’t want to have another surgery. Every doctor I went to, whether they were in spine care or rehabilitative medicine, all wanted to prescribe me medication,” he said. “I was having a lot of pain, but I couldn’t bring myself to take the medication they prescribed because I didn’t like the way it made me feel.”
At the recommendation of a friend, Saintvil went to Moss last summer where Saulino implanted the SPRINT system in his arm.

The needle used in the SPRINT system. / Courtesy
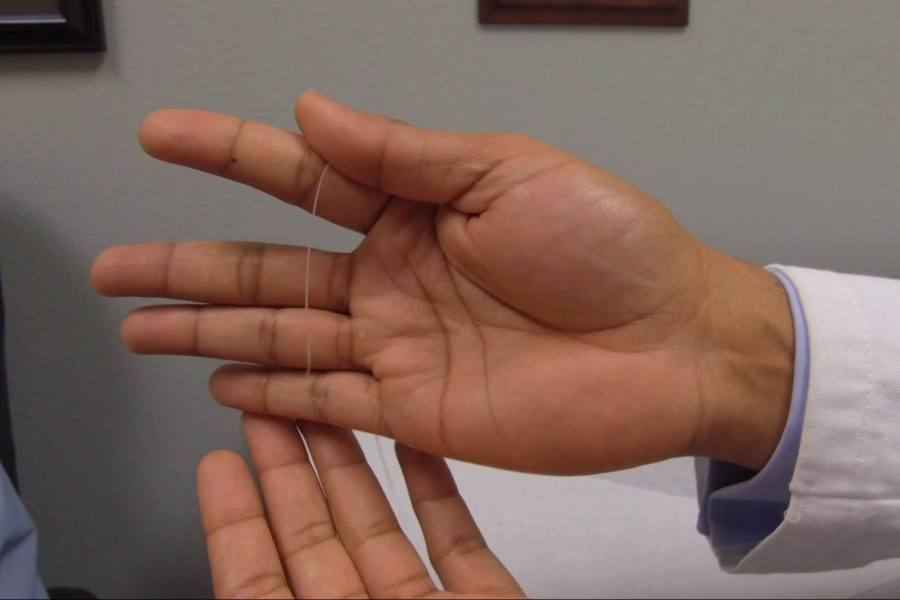
The SPRINT system relies on a strong but tiny wire that’s roughly the size of the fishing line. According to Saulino, the goal of the procedure is to get that wire close to nodes that are supporting the pain that the patient is experiencing.
To start, the doctor conducts an ultrasound or an x-ray, or, as in Peterson’s case, uses their hands and eyes to identify the right nodes to target. They then numb the skin before puncturing it with the needle to get close to the nodes they need to stimulate.
Next, the doctor advances the wire through the needle and then takes the needle out of the arm, leaving the wire in place. The wire comes out of the skin and gets connected to a cradle that connects to a battery pack. The patient is given a remote control that sends an electrical charge from the battery to the wire and ultimately to the targeted area where the patient is experiencing pain.
The tiny 0.3mm wire delivers small electrical impulses that activate nerves to reduce pain. / Courtesy
In total, Saintvil’s procedure took about an hour to complete. After 30 days, Saulino removed the system, and Saintvil says he’s been relatively pain-free ever since.
“After the first week, I felt relief,” Saintvil said. “They said I needed to have the treatment in for at least 30 days but after two weeks I didn’t feel any pain at all.”
According to Saulino, upwards of 50 to 70 percent of patients with stroke have shoulder pain. In clinical studies, SPRINT provided significant relief for 87 percent of participants experiencing chronic pain.
SPRINT has also been used in trials to treat post-amputation pain, shoulder pain, lower back pain, complex regional pain syndrome (CRPS), and post-operative pain following joint replacement. Based on positive trial results and encouraging outcomes from his own post-stroke pain patients, Saulino has plans to offer SPRINT as a treatment option for a broader patient population, including patients with low back pain.
The cost of therapies like SPRINT could be a barrier for some patients, however. Moss declined to share specific cost estimates with us saying costs vary widely depending on the price a hospital sets to perform the procedure and the insurance coverage a patient has. According to Saulino, hospitals that offer the treatment typically pay the upfront costs to purchase the implant and then the patient is billed through their insurance company. Some insurance companies will cover more of the cost than others. Neil Malhotra is an associate professor of neurosurgery at the Hospital of the University of Pennsylvania and co-director of the Translational Spine Research Lab at Penn Medicine. Malhotra cautioned that the technologies that make nerve stimulation therapies like SPRINT possible can be pricey, but he didn’t rule out offering the treatment to his patients at Penn.
“Sometimes insurance covers these treatments but often, they do not, which means the cost may fall to the patient,” he said. “Such a treatment would be low risk, with high potential benefit. If proven, we would consider offering this treatment at Penn.”
“Cost is such a difficult onion to peel,” Saulino added. “But if we can save one patient from opioid addiction, I’d say the cost is worth it.”